


How to Select a Binder for Toxic Indoor Mold Exposure: Addressing the Pros, Limitations & Nuances for Both Adults and Kids

Mycotoxins from old or new indoor mold growth are generally what make us “mold sick” when people think of “mold illness” and/or CIRS from a water damaged building. Mycotoxins require binders as the main therapy to get better (which I realize is a reductive statement but for simplicity purposes it is a mainstay of the healing care plan).
We don’t “kill” mycotoxins as they aren’t “alive” to “kill”
Mycotoxins are a toxin, not a pathogenic living organism; given this, mycotoxins need “removed” from the body; to do this we need to support our body in metabolic detoxification. In short, “detoxing” is the systematic process of “packaging up and shipping out toxins” that leave via our drainage pathways like sweating, peeing and pooping; note that the vast majority of toxins leave via stool. This is the high level overview of how most people “heal” from their current and/or former toxic indoor mold exposure. Big picture: we got to get the mycotoxins out of our system and our body needs assistance to do this well.
“Mold colonization” (versus mycotoxin bioaccumulation) is a different topic that is controversial.
Mold colonization is the process where mold becomes established and continues to grow within a living system, such as the human body, even after the initial exposure if the person left the exposure. You can actually see mold growing in a person’s nose on some test results of a MARCoNS nasal swab. Mold can also colonize in the lungs and in the gastrointestinal tract. Mold colonization is not the same as candida overgrowth, but both can occur simultaneously from a toxic indoor mold exposure. “Mold growing in the body” and “mycotoxins stored up in the body” are technically two different things that are end results of being exposed to mold.
To be clear, not everyone exposed to mold ends up with candida overgrowth. And not everyone with candida overgrowth has been exposed to mold. (Mold colonization and candida overgrowth are not one in the same but can go hand in hand).
But patients who have been exposed to toxic indoor mold can also develop candida overgrowth from the immunosuppressive mold exposure – which allows the candida to overgrow.
On a personal note, over the course of a couple years, I personally experienced this: oral thrush on my tongue and over 30 vaginal yeast infections before we figured out on a third opinion mold inspection that toxic mold was in our home driving my health problems (and my family’s health problems – which were all different from person to person).
We then remediated/small particle cleaned and I was able to go on and heal with a care plan that included antifungals to eradicate the overgrown candida; I also needed other therapies to detox the mycotoxins and resolve my CIRS diagnosis. The yeast infections did not come back thank god after we remediated!
Testing for Candida Overgrowth from Toxic Indoor Mold Exposure
Candida overgrowth from mold exposure is highly debated (I call it the “Mold Wars”); between the top Mold Illness Physicians, they debate over if these fungal pathogens needs “eradicated.” I tend to be more in the camp that we need to address candida overgrowth when it is present, while also addressing the root reasons as to WHY it overgrew. There are various tests to gauge this dysfunction in the body:
- OAT (organic acid testing)
- Candida antibody panel – can have false positives
- MARCoNS intranasal testing panel with fungal culture
- Vaginal Culture (to test for vaginal yeast infection)
- Tongue Scraping Culture (to test for oral thrush)
- Visually seeing candida growth on the body
- Even if it doesn’t perfectly fall into the confines of an ICD-10 code
- Often times oral antimicrobials and nasal sprays are needed for eradication aka “killing mold” or “candida overgrowth.”
- Antifungal usage is a separate topic from binders as they are each accomplishing something different, but felt I needed to spell it out. They can work synergistically together.
Note that sometimes people need both: Antimicrobials & Binders to Heal from the Various Ways Toxic Indoor Mold Can Harm the Body
Most people will need binders and some people will need antimicrobials IF there is a fungal burden to the body. Again, mycotoxin bioaccumulation and CIRS if applicable are not the same as mold/fungi colonization. The are not mutually exclusive.
Let’s focus on BINDERS for rest of this blog and removing mycotoxins from the body but wanted to speak to “mold colonization” first
I really like the CELLCORE drainage funnel as a visual and foundational explanation for how mycotoxins travel through the drainage pathways with the end goal to leave the body effectively with the assistance of a binder.
People need binders, especially when we have certain HLA haplotypes and/or have a high burden of toxins like mycotoxins in our body. This is because as our bile acids are “stingy” and most toxins easily recirculate enterohepatically. Note people have strong opinions on the Cellcore products (love or hate), but I do think it’s hard to argue the main principle of their graphic and high level overview of our bodily detox systems.
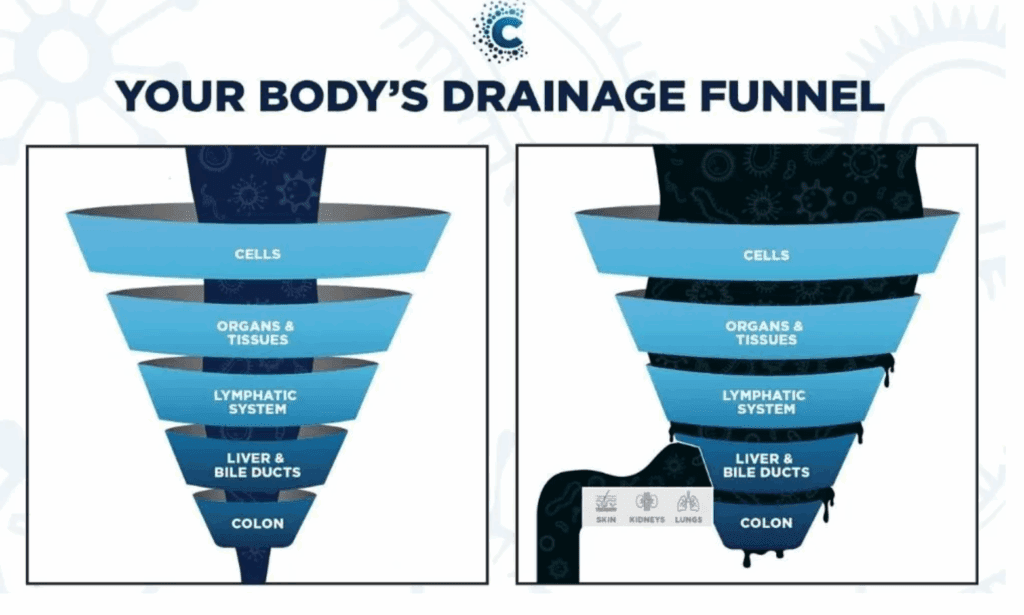
Toxins should “flow well” from the cells to lymph to blood to organs to elimination. If one kink in the assembly line is disrupted, the whole flow is disrupted.
The gut is often the the weakest link in the chain; if gastrointestinal function is suboptimal, toxins will not effectively leave as well. In a nutshell: gotta be regular with upper and lower gastrointestinal motility: aka pooping – as most mycotoxins will leave the body this way. This can often take needing extra support if you are living in mold:
- Oral magnesium supplements if constipated which happens (but the other extreme of diarrhea can happen too especially if the calprotectin is elevated)
- Topical castor oil packs over the abdomen
- Addressing low stomach acid and its root causes
- Screening for, finding and then eradicating overgrown gut pathogens
- Supporting bile flow as bile can get “sludgy” when there is a lot of mycotoxins; Phosphatidylcholine and cholagogues can be helpful
- There is a lot of nuance to all this – but picture: get the patient pooping 1-3x per day soft yet formed.
Generally once optimal gastrointestinal function is “underway” – this is an excellent time in add in oral binders – which is another big ol nuanced conversation.
What are oral binders?
Oral binders are medications or supplements taken by mouth that bind to specific substances (including mycotoxins) generally within the gastrointestinal (GI) tract, preventing them from being absorbed into the body. Now this is a blog, and doesn’t replace individualized medical advice, but here is some info below to point you in the right direction.
Remember: binding shouldn’t be arbitrary or random. It has a distinct purpose and we need to get a targeted plan in place with the end goal of the binder successfully:
- Increasing the MSH (if it’s low to get above 35)
- Flipping the VCS test back to negative
- Correcting other CIRS biomarkers if these are abnormal
- Other labs have normalized related to mold illness
- And then of course you are feeling better!
- I will also order “other downstream markers” to see that we are resuming optimal bodily levels that mold can deplete or alter (like vitamin D, iron, coq10, glutathione, mid luteal progesterone, thyroid antibodies, etc.)
Binders are a controversial topic in the mold world; let’s talk about this:
In a nutshell, binders do what they say they are going to do: they “bind” to mycotoxins (& other toxins and biotoxins) and help them be excreted from the body. Bile transport mycotoxins from the liver to gallbladder and through the GI tract and then the binder prevents the enterohepatic circulation of mycotoxins. Aka it helps the mycotoxins stay in the stool and leave the body with a bowel movement.
The controversy comes into play in regards to “which binder is the best?” Short answer? They are all able serve a purpose depending upon the scenario.
Binder options with Pros, Limitations and Nuances for Adults and Kids
- 1. Cholestyramine
- Dr. Ritchie Shoemaker, the pioneer of mold/CIRS illness research and treatment, recommends the use of cholestyramine for binding up mycotoxins and “taking them to the toliet.” Cholestyramine (CSM) is an FDA-approved medication used in an initial stage of the Shoemaker Protocol because it has a unique affinity for binding with biotoxins and effectively eliminating them from the body.
- CSM has been extensively tested in multiple clinical trials involving patients with chronic biotoxin illnesses. The benefit of using CSM has been confirmed by two double-blind, placebo-controlled crossover studies.
- In some patients, one month of CSM will increase the MSH biomarker and the make the VCS go from positive to negative assuming the person is out of the mold or biotoxin. For most people it takes multiple months or years of CSM (or other binders). CSM is not absorbed from the GI system—instead, it binds to cholesterol, bile salts, and biotoxins in the small intestine.
- With no additional exposures, CSM will remove all stored toxins from the body over time.
- Pros of cholestyramine
- Insurance may pay for it if prescribed by a Doctor
- Works faster compared to other binders as it has a high affinity for binding to mold and other biotoxins
- Evidenced based and been used for 20 years for treating mold illness and CIRS
- Both kids and adults can take it; kids just need smaller dose
- Limitations of cholestyramine
- Works in the gastrointestinal solely in regards to binding (not systemic)
- Not all mycotoxins are negatively charged (aflatoxin, tricothecenes, zearealnone, fusmosins) and consequently dont “need” a positively charged binder
- You have to find and pay a CIRS Physician willing to prescribe it; there are not many in the USA and I don’t think most of the these Providers take insurance
- Side effects: taking CSM can cause constipation, bloating or bowel discomfort and you are only detoxing well when you are pooping regularly
- Nutrient deficiencies: this bile acid sequestrant can interfere with the absorption of several micronutrients, particularly the fat-soluble vitamins A, D, E, and K. It can also impact the absorption of folate. Additionally, studies suggest that cholestyramine may decrease the absorption of certain minerals like iron, magnesium, and zinc
- There is an online place to get cholestyramine prescribed by a provider but this does not replace medical evaluation and management. I have it linked in my online program.

- 2. Welchol
- Welchol is another prescription binder option similar to cholestyramine but “less strong.” Welchol (colesevelam) is a prescription medication used to lower “bad” cholesterol (LDL) and improve blood sugar control in adults with type 2 diabetes. It is a bile acid sequestrant that works in the intestines. It is often seen as another option in the Shoemaker Protocol especially if a person is unable to tolerate cholestyramine. Welchol should not be used in individuals with high blood triglyceride levels (over 500 mg/dL), a history of pancreatitis caused by high triglycerides, or intestinal blockage
- Pros of Welchol
- Usually better tolerated by some if can’t tolerate cholestyramine
- Something to swallow as a pill if you don’t do well with powders in liquid
- Kids could take if able to swallow pills
- Limitations of Welchol
- Note that welchol is a step down from cholestyramine in terms of it not able to “bind as much as fast.”
- Welchol is about 1/4 of the power of cholestyramine in terms of ability to bind biotoxins so it will take longer
- Usually more money than cholestyramine
- Need to have access to someone who will prescribe it for you
- Welchol is another prescription binder option similar to cholestyramine but “less strong.” Welchol (colesevelam) is a prescription medication used to lower “bad” cholesterol (LDL) and improve blood sugar control in adults with type 2 diabetes. It is a bile acid sequestrant that works in the intestines. It is often seen as another option in the Shoemaker Protocol especially if a person is unable to tolerate cholestyramine. Welchol should not be used in individuals with high blood triglyceride levels (over 500 mg/dL), a history of pancreatitis caused by high triglycerides, or intestinal blockage

3. Okra & Beets as a food based binder
- Okra and beets are plant based foods that we can consume in concentrated doses that has about the same effectiveness by itself as Welchol! How cool is that. There are two good options I am aware of and use with patients:
- Mycobind powder – which I have linked in the protocol of my online healing from mold program. Mycobind is a blend of okra and beets crushed up into a powder form – it is about half as strong as cholestyramine in terms of ability to bind to bile acids (which transport mycotoxins to the GI tract). It can be easily added to water and you drink one scoop 1 to 4 times per day if you can tolerate. Or another option is the two below combined together:
- Alovea limitless beet capsules – beets are second to okra in terms of food binders. Beets are a high oxalate containing food so many can’t tolerate. I took this beet supplement (2 capsules per day) as the betalains are extracted and thus oxalates are drastically reduced. This can also help reduce MMP9 and tgfbeta1
- Earthborn Okra capsules – 4 capsules is comparable to 4 scoops of mycobind each day.
- Pros of okra and beets as food and supplement based binders
- Is cheaper depending upon insurance cover of prescription binders
- Don’t need a prescription
- Accessible to people to buy online
- Is studied as effective
- Betalains found in the alovea Limitless supplement have other benefits: can lower MMP9 and tgfbeta1 and help reduce oxidative stress which is helpful for those with elevated levels of these inflammatory markers
- Cons of okra and beets
- Will take longer than cholestyramine.
- Another possible con is okra has oxalates, and some mold exposed people do not tolerate oxalates especially if they have candida overgrown in the body.
- Oxalates in EXCESS can contribute to kidney stones. Most humans who consume oxalates metabolize them with no problem; the food is usually the straw breaking the camel’s back and the bigger issues are sometimes the candida burden that is off putting all the extra oxalates. Don’t take mycobind or okra or beets if you have kidney stones
- Candida may need addressed first (if applicable) before someone can tolerate okra.

In the CIRS community, the 3 options above are the most agreed upon binders.
However, mold illness is more than CIRS (which not everyone has when they are exposed to mold or biotoxins) and there are many other binders out there that are researched and anecdotally many people get better with other over the counter binders especially if they tolerate these ones below:
4. Some example of other supplement binders include clays, modified citrus pectin, humic and fulvic acid, charcoal, zeolites to name a few. See this chart below:

- Pros of other over the counter binders:
- Don’t need to pay a physician to prescribe as cost & accessibility is a huge barrier with prescription binders
- Many will bind to other toxins like heavy metals and many other common indoor molds
- Kids can take most of these above and some are available in liquid and chewable form
- Liquid, water based and tasteless TRS (toxin removal spray) can be given to infants and this is what we gave to my son as it was what he was willing to swallow as a toddler. Sometimes you have to do something as it is better than nothing. General dosing is 1 spray for every 30 lbs; we even give it to our cats
- Pectasol chewables (linked here in Fullscript 15% off and free shipping) can also be given to young children or open up capsules and put in applesauce for other children)
- Some over the counter binders work systemically like fulvic acid and the brand Cellcore has carbon based technology and can cross cell membranes and able bind toxins that are in tissues, not just the ones that have made it to the GI tract. Get Cellcore Biotoxin Binder here with code: 2FQLrpNb to access to the website.
- Cons of various over the counter binders
- Dr. Shoemaker’s research argues the positive charged binders work best on negative charged mycotoxins which is ONE factor that influences binder efficacy but other research shows there are more factors that influence “bindability.” But various binders can “attract” mycotoxins via multiple mechanisms besides just looking at “charge:” hydrophobic binding, ionic based binding, chelation based binding and physical encapsulation.
- I myself healed my CIRS the first time with over the counter products and have seen it happen in patients but the research to date says prescription binders work best and faster.
At the end of the day when selecting a binder after weighing all this information:
- I think some binding is better than no binding
- Ultimately you have to go with what the patient can tolerate
- Go with what you have access too and can afford
- Use a binder that still allows one to 3 bowel movements as you will only be detoxing well if there is regular bowel movements each day.
Binding mycotoxins and taking them to the toliet is typically a many month journey; but the time will pass anyways so might as well do the right thing and get them out over time and start feeling better!
Little by little, day by day, these health deterrents will leave the body with binders and you CAN get better from mold and/or biotoxin related health problems.
Happy binding!
Need more assistance, protocols, databases and context of how binders fit into the big picture? Take my online Healing from Mold Online Program for a step by step framework so you miss no major components of “shutting off the faucet and draining the tub.”

